Merit Medical ProGuide Chronic Dialysis Catheter User Manual
Page 7
syringe, IV tubing, or bloodlines.
• Close all clamps in the center of the extension tubing. Repeated clamping near or on the luer lock
connectors may cause tubing fatigue and possible disconnection.
• Clamping of the tubing repeatedly in the same location may weaken the tubing. Extension tubing may
develop cuts or tears if subjected to excessive pulling or contact with rough edges.
POST DIALYSIS HEPARINIZATION
Follow institutional protocol for heparin concentration. If the catheter is not to be used immediately for
treatment, follow the suggested catheter patency guidelines.
1. Draw the heparin / saline solution into two syringes, corresponding to the amount designated on the
arterial and venous extension tubing clamp. Assure that the syringes are free of air.
2. Attach a syringe containing heparin solution.
3. Open the extension tubing clamp.
4. Aspirate to ensure that no air will be forced into the patient.
5. Inject the heparin solution into each lumen using a quick bolus technique.
PRECAUTION: To maintain patency between treatments, a heparin lock must be created in each
lumen of the catheter.
6. Close extension clamps.
PRECAUTION: Extension clamps should only be open for aspiration, flushing, and dialysis treatment.
7. Remove syringes.
PRECAUTION: In most instances, no further heparin flush will be necessary for 48-72 hours, provided
the lumens have not been aspirated or flushed.
8. Assure luers are capped.
CATHETER PERFORMANCE PRIMING VOLUMES
• The priming volumes of both the arterial and venous lumens are printed on each extension
tubing clamp.
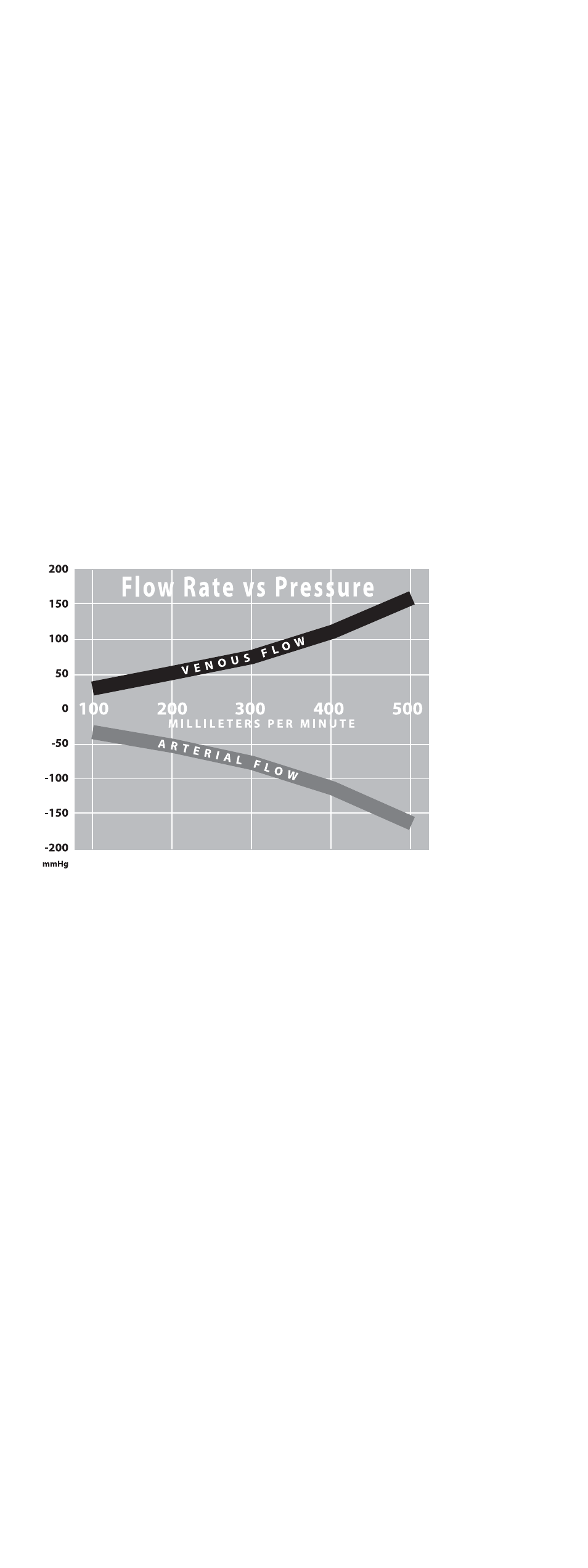
FLOW RATE
• Typical flow rate vs. pressure with the ProGuide 14.5 FR X 28 cm (tip to hub)
catheter (with side holes)
TROUBLESHOOTING INSUFFICIENT FLOWS
Treatment for insufficient flow will be at the discretion of the physician. Excessive force should not be used
to flush an obstructed lumen. Insufficient blood flow may be caused by an occluded lumen due to clotting
or fibrin sheath or because the arterial hole is contacting the vein wall. If manipulation of the catheter or
reversing arterial and venous lines does not help, the physician may attempt to dissolve the clot with a
thrombolytic agent.
MANAGEMENT OF ONE-WAY OBSTRUCTIONS
One-way obstructions exist when a lumen can be flushed easily but blood cannot be aspirated. This condi-
tion is usually caused by tip malposition. One of the following adjustments may resolve the obstruction:
• Reposition the catheter
• Reposition the patient
• Have the patient cough
• Provided there is no resistance, flush the catheter vigorously with sterile normal saline to try to move
the tip away from the vessel wall.
INFECTION
Catheter related infection is a serious concern of indwelling catheters. Follow institutional protocol when
removing the catheter.