Merit Medical Embosphere Microspheres Prefilled Syringe IFU-US User Manual
Page 6
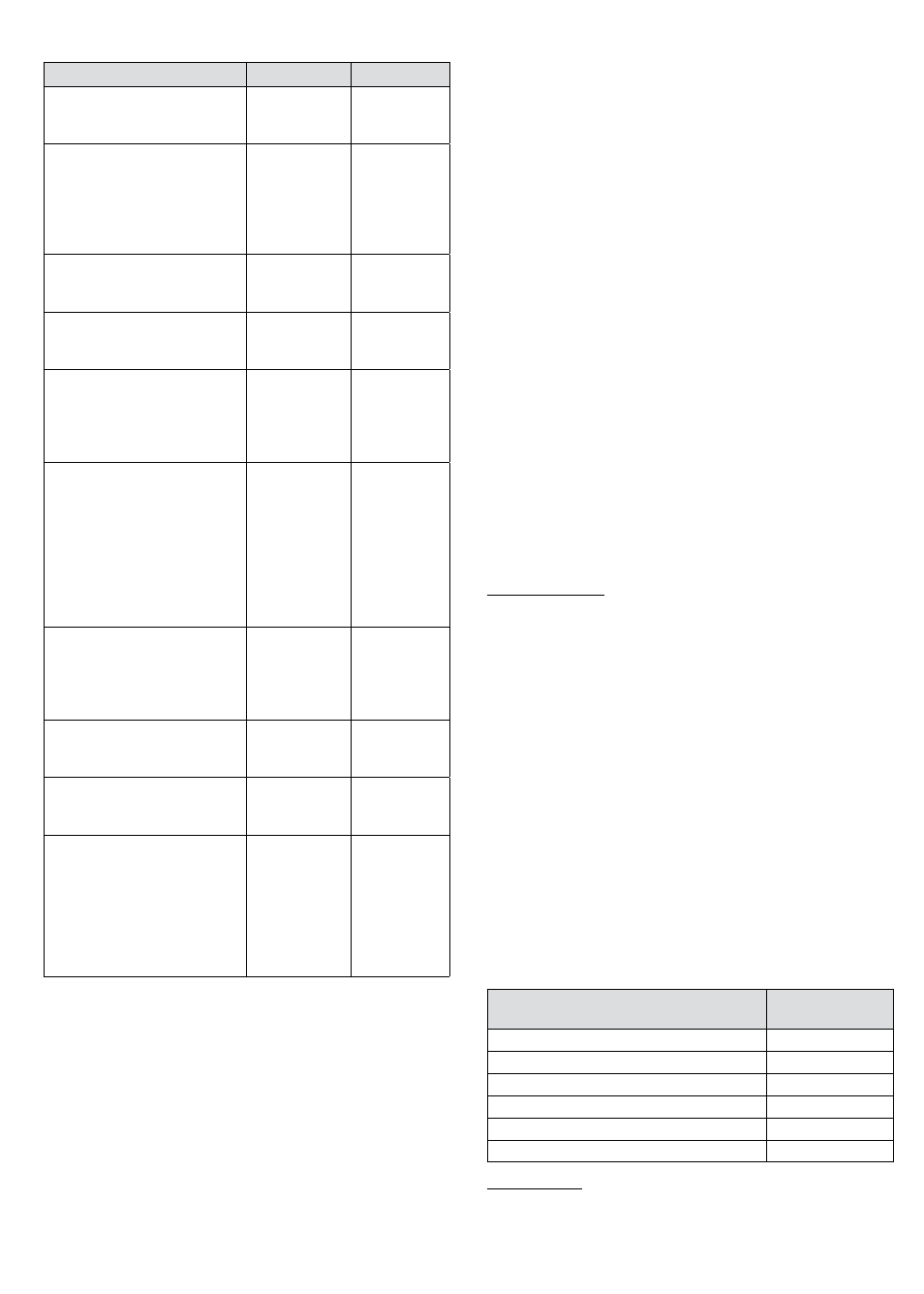
Table 1- Patient Demographics
UFE
Hysterectomy
AGE IN YEARS
Mean (SD)
Range
42.4 (4.2)
30-50
41.6 (5.3)
31-50
ETHNIC ORIGIN
Asian/Pacific Island
African American
Hispanic
Caucasian
Other
1 (1%)
67 (59%)
7 (6%)
35 (31%)
3 (3%)
2 (4%)
9 (18%)
8 (16%)
31 (62%)
0 (0%)
HEIGHT (cm)
Mean (S.D.)
Range
159.9 (10.5)
131-186
161.8 (10.1)
132-178
WEIGHT (kg)
Mean (S.D.)
Range
72.7 (16.2)
46-123
75.1 (21.5)
50-146
MENSTRUAL STATUS
Frequent
Infrequent
Regular
Unknown
8 (8%)
1 (1%)
93 (91%)
0 (0%)
14 (28%)
2 (4%)
33 (66%)
1 (2%)
PRIOR FIBROID TREATMENT
None
GnRH agonist
Oral contraceptive
Other hormonal
Myomectomy
D & C
Hysteroscopy
Other invasive
53 (52%)
9 (9%)
25 (25%)
9 (9%)
20 (20%)
17 (17%)
13 (13%)
9 (9%)
35 (70%)
2 (4%)
5 (10%)
5 (10%)
4 (8%)
1 (2%)
2 (4%)
3 (6%)
NUMBER OF FIBROIDS
1
2
≥ 3
no response
28 (25%)
37 (33%)
48 (42%)
0 (0%)
20 (40%)
19 (38%)
10 (20%)
1 (2%)
UTERINE VOLUME (cc)*
Mean (SD)
Range
692.4 (462.8)
185.6-3076.3
389.2 (521.2)
91.8-3415.1
DOMINANT FIBROID VOLUME (cc)
Mean (SD)
Range
147.4 (154.3)
5.1-776.8
90.6 (354.8)
3.2-2322.3
FIBROID TYPE
Intramural
Subserosal
Submucosal
Transmural
Pedunculated
More than one type indicated for
some patients
69 (61%)
20 (18%)
18 (16%)
11 (10%)
2 (2%)
32 (64%)
8 (16%)
13 (26%)
1 (2%)
4 (8%
*Eighty-four percent of the UFE patients and 98% of the
hysterectomy patients had baseline uterine volumes of 1000 cc
or less.
Study Results
The study results are presented below for 107 patients considered
to be in the Phase II UFE study cohort, which consisted of 11 UFE
Phase I patients who met the Phase II eligibility criteria and 96
evaluable UFE Phase II patients.
Procedure, Discharge, and Recovery Information
All UFE procedures were technically successful with no
intraoperative complications that prevented completion of
the procedure. The majority (77%) of the UFE procedures were
performed using a 5 Fr catheter with either a 4 Fr (19%) or 3 Fr (3%)
in the remainder. Seventy-two patients were treated with 500-700
micron spheres, 66 patients with 700-900 micron spheres and 18
patients with 900-1200 micron spheres. Many of the patients
were treated with more than one sphere size. The most common
treatment approach was to start with a smaller sphere size and
then to increase the size if necessary. The volume of spheres
required varied inversely with the sphere size as an average of 7.2
cc of 500-700 micron spheres was used as compared to 6 cc of 700-
900 micron spheres and 4.1 cc of 900-1200 micron spheres.
The majority of UFE patients underwent the procedure while
under conscious sedation with a local anesthetic given at the
puncture site. No UFE procedures were performed under general
anesthesia. The average UFE procedure time from first arterial
puncture to final catheter removal was 58 ± 28 minutes (range 10-
140 minutes). By comparison, all of the hysterectomy surgeries
were performed under general anesthesia, regardless of the type
of hysterectomy performed, and the average surgery time from
skin incision to skin closure was 93 ± 38 minutes (range 35-171
minutes) (p<0.001). The majority of the hysterectomy procedures
were done abdominally (76%).
Eighty-seven percent of the UFE patients were discharged from
the hospital on the day following the embolization procedure
and 12% on the same day as the procedure. Hysterectomy
patients spent a significantly longer time in the hospital (p<0.001),
with an average stay of 2.3 days as compared to 0.9 days for the
UFE patients. UFE patients were back to work in an average of
10.7 days, however, this took an average of 30.7 days for the
hysterectomy patients (p<0.001). Similarly, the UFE patients
returned to normal daily activities more than three times quicker
than the hysterectomy patients (mean 10.9 days for UFE versus
37.4 days for hysterectomy, p<0.001).
Primary Efficacy Endpoints
Menstrual Bleeding
To be eligible for UFE in this study, patients were required to have
abnormally heavy menstrual bleeding, with a baseline score of ≥
150 on the Pictorial Bleeding Assessment Chart (PBLAC) of Janssen
et al. (1995). Success was defined as ≥ 50% reduction in PBLAC
score by the 6-month follow-up evaluation. Additional measures
were also used to assess changes in menstrual bleeding, including
patient self-assessment of their bleeding level and a menorrhagia
questionnaire.
Changes in menstrual bleeding generally occurred quickly
following UFE, with 92% of the patients showing some
improvement by 3 months. Table 2 presents the menstrual
bleeding success rates at 6 months in the intent-to-treat
population. The data in Table 2 reflects completed PBLACs from
90 of the 107 Phase II UFE patients (84%). Six patients (6%) did
not complete a 6-month PBLAC because they were either lost
to follow-up (n=4) or had a hysterectomy (n=2) prior to this
evaluation period. The eleven remaining patients (10%) without
6-month PBLAC scores had sufficient information from the other
menstrual bleeding assessments to determine their level of
success on this endpoint.
Table 2 - Efficacy: Menstrual Bleeding Success Rates in Intent-
to-Treat Population
% Reduction From Baseline
6 Months
N/107 (%)
≥ 50%
69 (65%)
30-49%
15 (14%)
0-29%
7 (7%)
< 0%
10 (9%)
Lost to Follow-up
4 (4%)
Hysterectomy prior to 6 months
2 (2%)
Bulk Symptoms
A fibroid-specific symptom questionnaire was used to assess
changes in three fibroid-related symptoms, pelvic pain, pelvic
6