Merit Medical Centros FLO IFU User Manual
Page 4
• The catheter should be accessed or have site care only when the
staff and patient wear a mask and the staff wears clean gloves.
• Clamping of the tubing repeatedly in the same location may
weaken tubing. Avoid clamping near the luers and hub of the
catheter.
• Do not use sharp instruments near the extension tubing or
catheter lumen.
• Repeated overtightening of blood lines, syringes, and caps will
reduce connector life and could lead to potential connector failure.
• Use only luer lock (threaded) connectors with this catheter.
• Examine catheter lumen and extensions before and after each
treatment for damage.
• To prevent disconnections, assure the security of all caps
and bloodline connections prior to and between treatments.
• Excessive force should NOT be used to flush obstructed lumen.
DO NOT use a syringe smaller than 10 ml (cc).
• Do not use scissors to remove dressing.
INSERTION SITES:
The right internal jugular vein is the primary anatomical location
for chronic dialysis catheters. However, the left internal jugular vein,
as well as the external jugular veins and subclavian veins can also
be a consideration. As with all invasive procedures, the physician
will assess the anatomical and physiological needs of the patient to
determine the most appropriate catheter entry site. The catheter is
available in various lengths to accommodate the varying anatomical
differences of patients as well as the differences between right and
left side approaches.
RIGHT INTERNAL JUGULAR VEIN
• The patient should be in a modified Trendelenburg position, with
the upper chest exposed and the head turned slightly to the side
opposite the insertion area. A small rolled towel may be inserted
between the shoulder blades to facilitate the extension of the
chest area.
• Have patient lift his/her head from the bed to define the sterno-
cleidomastoid muscle. Catheterization will be performed at the
apex of a triangle formed between the two heads of the sterno-
cleidomastoid muscle above the clavicle. The carotid artery should
be palpated medial to the point of catheter insertion.
• Using ultrasound, ensure the jugular vein is patent and distendent.
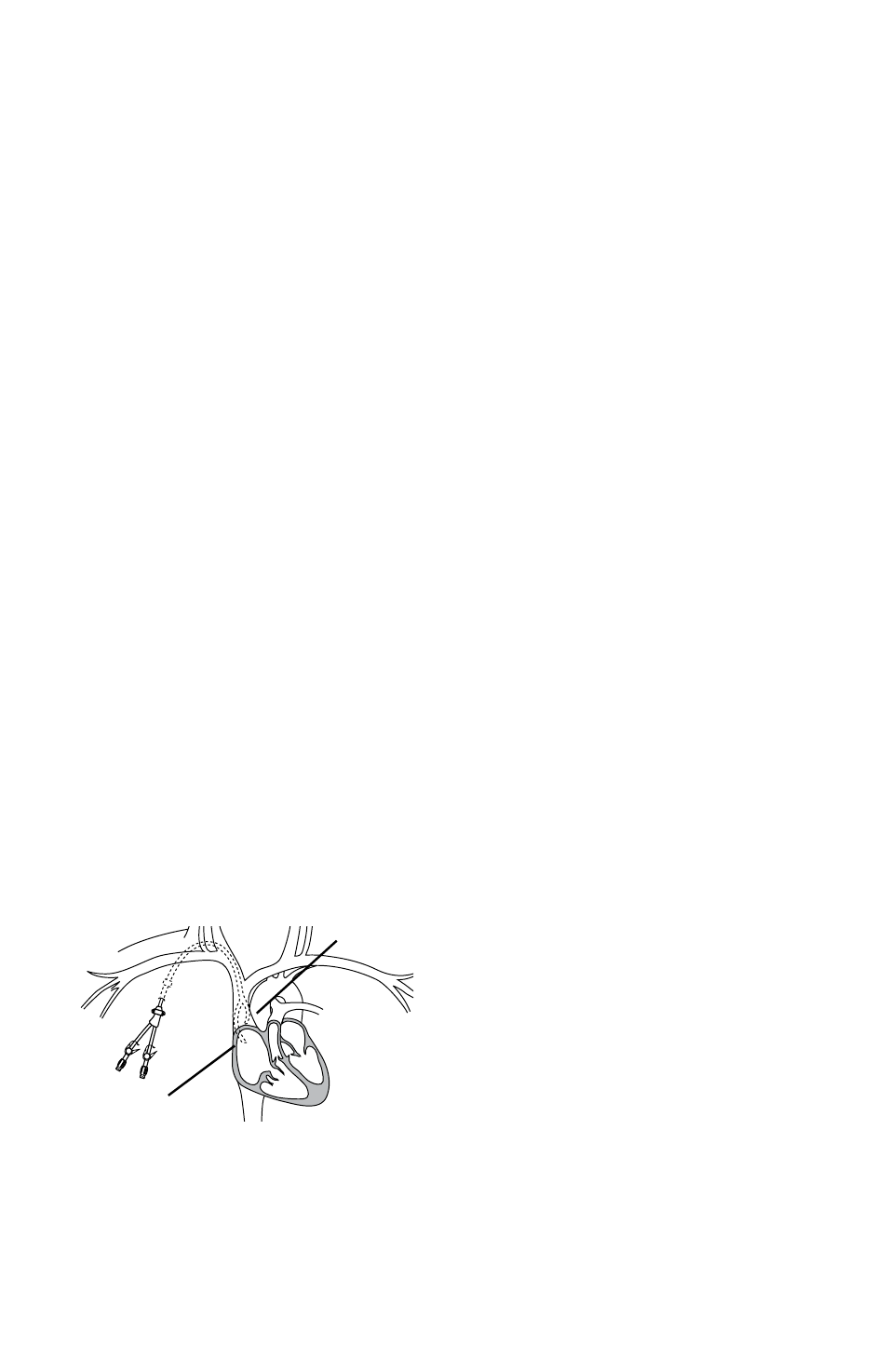
The Centros & CentrosFLO should always be placed so that the end
of the arterial lumen (shorter tip) is positioned towards the patient’s
left, as shown below. This allows the venous tip to curve away from
the lower vena cava and right atrial wall. For catheters placed through
the right IJ, this means that the arterial hub is on the upper and outer
side of the curving catheter. For catheters placed through the left IJ,
the arterial hub is on the lower and inner side of the catheter.
• Confirm final position of catheter with chest x-ray or fluoroscopy.
Routine x-ray should always follow the initial insertion of this
catheter to confirm proper tip placement prior to use. To optimize
self-centering tip design, the contact point of the curved arterial tip
should be positioned in the lower third of the vena cava, with the
venous tip in the right atrium or at the junction of the right atrium
and superior vena cava. Alternatively, both tips of the catheter may
be placed in the right atrium under fluoroscopy as recommended
by the 2006 Kidney Disease Outcomes Quality Initiative (KDOQI)
guidelines.
WARNING:
• Patients requiring ventilator support are at increased risk of
pneumothorax during subclavian and Jugular vein cannulation,
which may cause complications.
DIRECTIONS FOR SELDINGER INSERTION USING A PEELAWAY
INTRODUCER:
K-DOQI Guidelines recommend the use of ultrasound guidance and
fluoroscopy for placement NOTE: Mini access (“micropuncture”) is
recommended. Follow manufacturer’s guidelines for proper insertion
technique.
• Read instructions carefully before using this device. The catheter
should be inserted, manipulated, and removed by a qualified,
licensed physician or other qualified health care professional under
the direction of a physician.
• The medical techniques and procedures described in these
Instructions For Use do not represent all medically acceptable
protocols, nor are they intended as a substitute for the physician’s
experience and judgment in treating any specific patient.
• Use standard hospital protocols when applicable.
1. Strict aseptic technique must be used during insertion, mainte-
nance, and catheter removal procedures. Provide a sterile operative
field. Use sterile drapes, instruments, and accessories. Shave the skin
above and below the insertion site. Perform surgical scrub. Wear
gown, cap, gloves, and mask. Have patient wear mask.
2. The selection of the appropriate catheter length is at the sole
discretion of the physician. To achieve proper tip placement, proper
catheter length selection is important. Routine x-ray should always
follow the initial insertion of this catheter to confirm proper place-
ment prior to use.
3. Administer sufficient local anesthetic to completely anesthetize the
insertion site.
4. Determine site for needle entry into vein. Insert the introducer
needle with attached syringe into the target vein using ultrasound in
real time if possible. Aspirate to ensure proper placement in vein.
PRECAUTION: If arterial blood is aspirated, remove the needle and
apply immediate pressure to the site for at least 15 minutes. Ensure
that the bleeding has stopped and that no hematoma has developed
before attempting to cannulate the vein again.
5. Remove the syringe and place thumb over the end of the needle
to prevent blood loss or air embolism. Draw flexible end of guidewire
back into advancer so that only the end of the guidewire is visible.
Insert advancer’s distal end into the needle hub. Advance guidewire
with forward motion into and past the needle hub into the target
vein. Observe progress of the wire with fluoroscopy when possible
and advance the wire into the superior vena cava.
CAUTION: Monitor patient for arrhythmia throughout this procedure.
Cardiac arrhythmia may result if guidewire is allowed to pass into
the right atrium or ventricle. The guidewire should be held securely
during this procedure.
CAUTION: Do not advance the guidewire or catheter if unusual
resistance is encountered.
PRECAUTION: The length of the guide wire inserted is determined by
the size of the patient and the anatomical site used.
6. Remove needle and leave guidewire in the vena cava.
7. Make a small secondary incision at the exit site on the chest wall
below the clavicle. Make the incision at the exit site wide enough to
accommodate the catheter and dilate skin with hemostats.
8. Irrigate catheter with saline, then clamp catheter extension sets to
ensure that the saline is not inadvertently drained from lumens.
arterial
venous