Defibtech DDU-120 Series User Manual
Page 58
50
DAC-530E-EN-BH
8.1.6.2 Methods
AEDs were prospectively randomized according to defibrillation waveform on a daily basis in four
emergency medical services systems. First responders used either the 150-J biphasic AEDs
or 200- to 360-J monophasic waveform AEDs on victims where defibrillation was indicated. A
sequence of up to three defibrillation shocks was delivered: 150J-150J-150J for the biphasic units
and 200J-200J-360J for the monophasic units. Defibrillation was defined as termination of VF for >
5 seconds, without regard to hemodynamic factors.
8.1.6.3 Results
Of 338 patients with an out-of-hospital cardiac arrest, 115 had a cardiac etiology, presented with
ventricular fibrillation, and were shocked with one of the randomized AEDs. There were no
statistical differences between the monophasic and biphasic groups in terms of age, sex, weight,
primary structural heart diseases, cause or location of arrest, bystanders who witnessed the arrest,
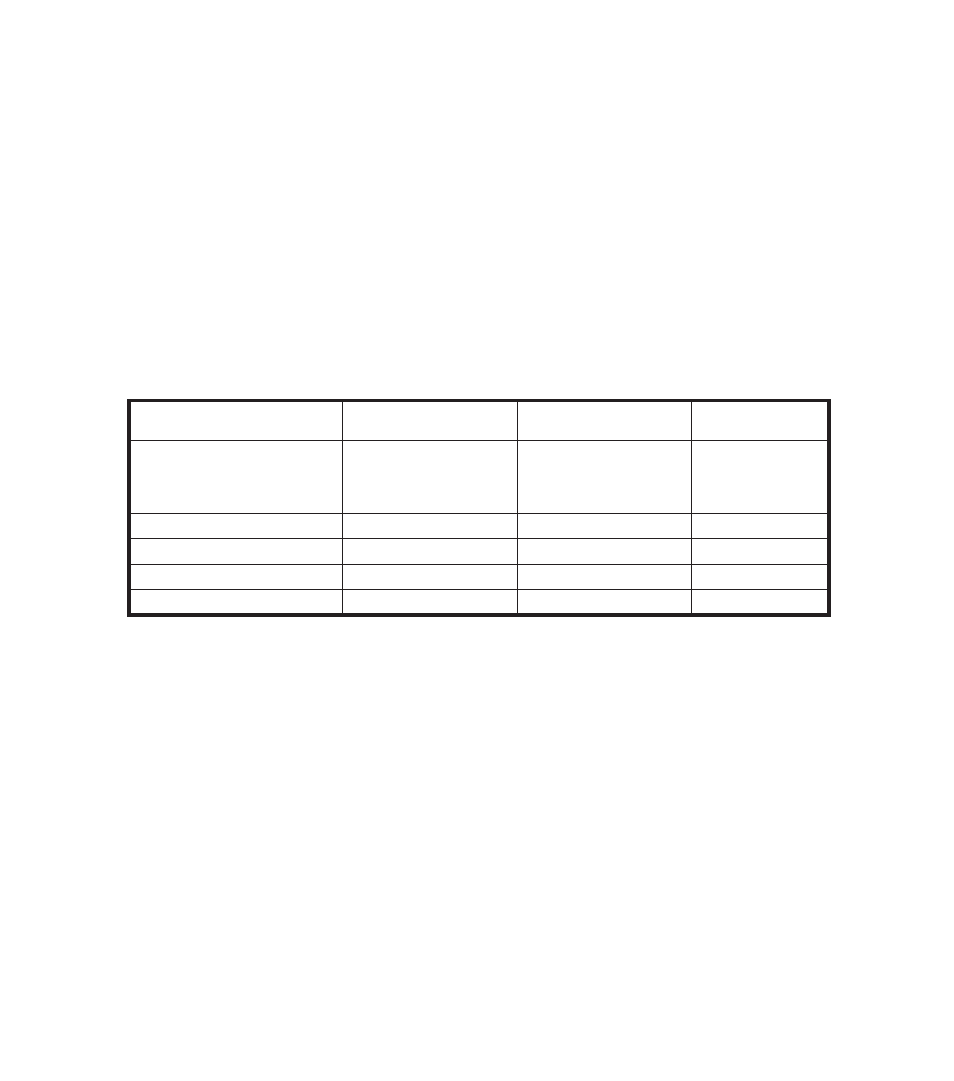
or type of responder. A summary of the results is presented in table below.
Biphasic Patients
Number (%)
Monophasic Patients
Number (%)
P Value
Defibrillation Efficacy:
1 shock
< 2 shocks
< 3 shocks
52/54 (96%)
52/54 (96%)
53/54 (98%)
36/61 (59%)
39/61 (64%)
42/61 (69%)
< 0.0001
< 0.0001
< 0.0001
Patients defibrillated
54/54 (100%)
49/58 (84%)
0.003
ROSC
41/54 (76%)
33/61 (54%)
0.01
Survival to Hospital Admission
33/54 (61%)
31/61 (51%)
0.27
Survival to Hospital Discharge
15/54 (28%)
19/61 (31%)
0.69
8.1.6.4 Conclusion
More patients were defibrillated with an initial biphasic shock than monophasic shock and
ultimately the biphasic waveform defibrillated at higher rates than the monophasic waveform. A
higher percentage of patients achieved Return Of Spontaneous Circulation (“ROSC”) after biphasic
shocks. Rates of survival to hospital admission and discharge did not statistically differ between
the two waveforms.